About the Use of Dipsticks to Diagnose UTI
No patient over 65 years old of any sex should have a dipstick done for any reason for the diagnosis of UTI
Women under 65 years old should only have dipstick if required after:
- Excluding vaginal and urethral causes of urinary symptoms AND
- Patient should have at least one of the 3 key diagnostic signs/symptoms of dysuria (burning sensation on passing urine),NEW nocturia and urine cloudy to the naked eye.
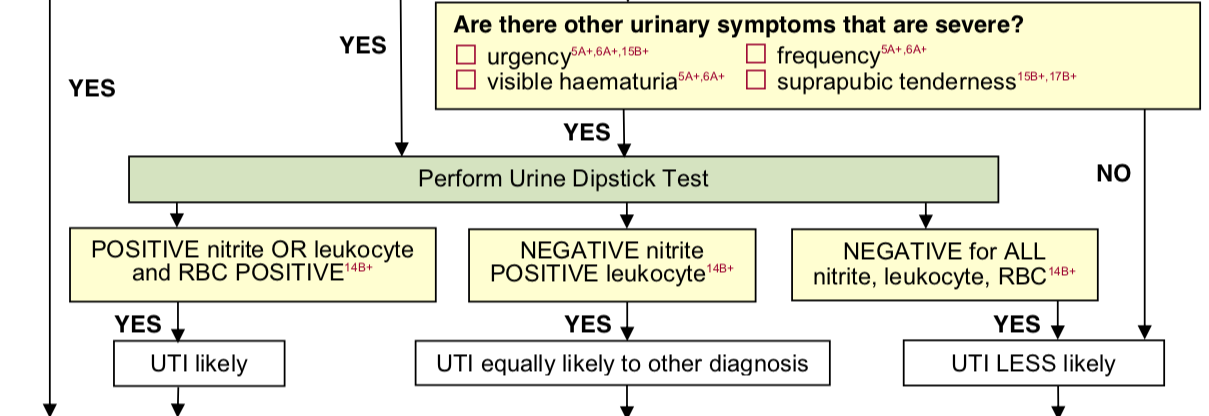
Please refer to the RCGP flow chart copied below and in full version in links on right


MSU should be be sent but dipstick NOT performed when patient presenting with UTI symptoms is:
- Male
- Over 65 (male or female)
Guidelines for diagnosis and treatment of UTI in catheterised patients
-
Look for systemic symptoms when suspecting UTI: pyrexia >38, hypotension, new or increased confusion, loss of diabetic control
- Collect catheter specimen CSU appropriately.
-
NO DIPSTICK is necessary as this will usually be positive regardless of UTI.
-
Send specimen to lab, labelling clearly that this is a CSU specimen and treat empirically for UTI
NB: Bacteriuria is an inevitable consequence of long term (>5days) catheterisation. Unless the patient has symptoms of infection, do not send a specimen.
Recurrent UTI
3 or more proven UTIs within 12 months should be referred to Urology
Recurrent UTI with Urease producing bacteria eg Klebsiella, Proteus mirabilis should be referred to Urology due to increased risk of forming Staghorn Calculi
Persistent microscopic haematuria in over 50s
Should be referred via the 2WW pathway to urology
(Visited 15,756 times, 1,119 visits today)
Leave feedback
You must be logged in to post a comment.