Abnormal Potassium Results
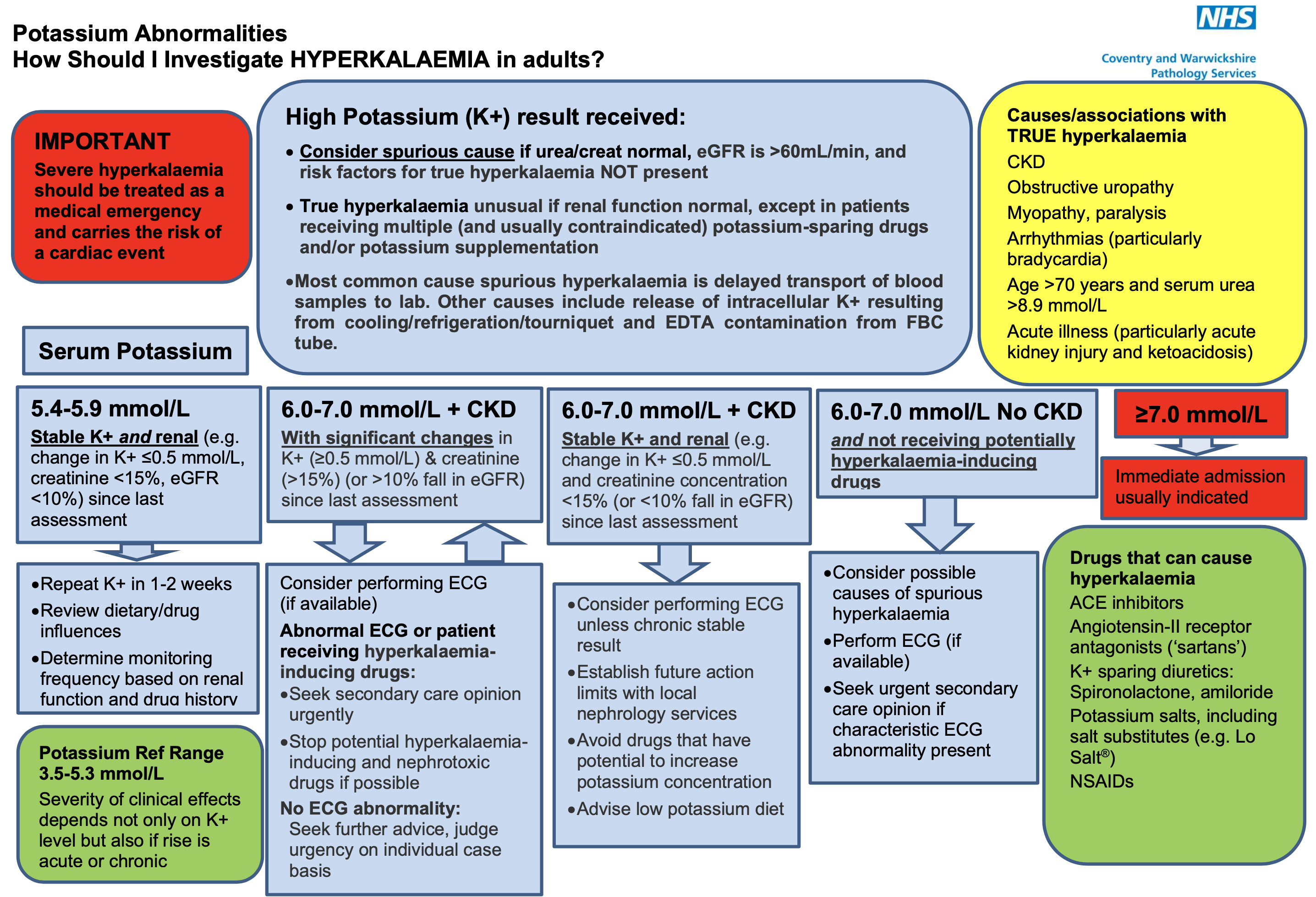
High Potassium (K+) result received:
Consider spurious cause if urea/creat normal, eGFR is >60mL/min, and risk factors for true hyperkalaemia NOT present.
True hyperkalaemia unusual if renal function normal, except in patients receiving multiple (and usually contraindicated) potassium-sparing drugs and/or potassium supplementation.
Most common cause spurious hyperkalaemia is delayed transport of blood samples to lab.
Other causes include release of intracellular K+ resulting from cooling/refrigeration/tourniquet and EDTA contamination from FBC tube.
Low Potassium (K+) result received:
If cause is obvious: Investigate and treat any underlying cause such as diarrhoea. Consider potassium replacement treatment
If cause is unclear: Review medication for drugs known to cause hypokalaemia.
Consider nutritional status and dietary potassium intake
Low magnesium can cause hypokalaemia.
Consider testing random urine potassium:creatinine ratio, >2.5 mmol/mmol suggests renal loss ·
If hypertensive, consider need for renin-aldosterone studies.
Consider ectopic ACTH production (typically from small cell lung carcinoma), particularly if severe or rapidly developing.

Abnormal Sodium Results
High Sodium (Na) result received:
Establish history of thirst, fluid intake/loss and current treatments.
Check for clinical features of dehydration and/or hypovolaemia.
Repeat sodium to confirm and establish if acute and changing or chronic and stable.
Changes of up to 4 mmol/l can reflect non‐ significant variation.

Low Sodium (Na) result received:
Establish history of fluid intake and current treatments.
Assess fluid status to identify if hypovolaemic or hypervolaemic.
Repeat sodium to confirm and establish if acute and changing or chronic and stable.
Changes of up to 4 mmol/l can reflect non‐ significant variation.

Leave feedback
You must be logged in to post a comment.