Abnormal Liver Function Tests
Chronic liver disease is often asymptomatic until later stages when complications arise.
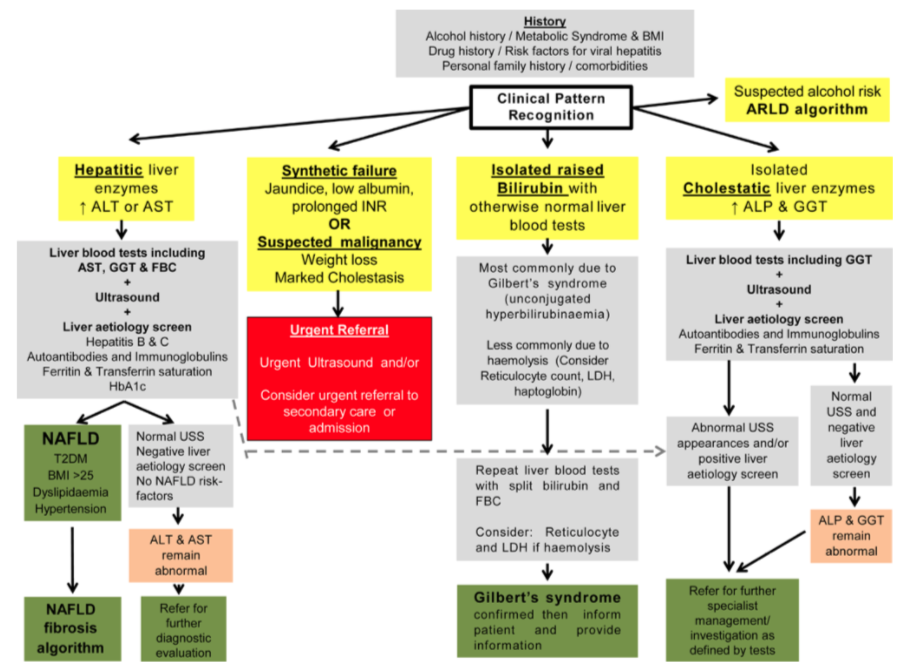
Mild abnormalities of either ALT or ALP are common in general practice and may be transient, but appropriate investigation should not be overlooked as this may lead to missed opportunity for early intervention.
The commonest reasons are alcohol and fatty liver.
Patients with jaundice or with clinical evidence of liver failure require urgent referral. For others, address lifestyle issues (alcohol, diet, weight), review medications, and exclude viral hepatitis. If liver enzymes remain abnormal after 3 months, further investigation is appropriate with full liver screen and ultrasound scan.
Pre-referral investigations: Routine referrals will not be accepted without a liver screen and ultrasound. See algorithm for management of abnormal liver enzymes.
Referral threshold: Consider referral to a hepatology clinic if multiple enzymes are raised, if there is diagnostic doubt or if there is clinical concern of cirrhosis
Mild abnormalities of ALT or ALP are common and may be transient, but appropriate investigation should not be overlooked as this may lead to missed opportunity for early intervention.
The commonest reasons are alcohol and fatty liver. Lifestyle issues (alcohol, diet, weight) should be addressed, medications reviewed and viral hepatitis should be excluded. If liver enzymes remain abnormal after 3 months, a full liver screen is appropriate. Consider referral to a hepatology clinic if multiple enzymes are raised, enzymes consistently twice the upper limit of normal or there is clinical concern of cirrhosis.
Alcohol Dependency
Patients with alcohol dependency should be directed to community alcohol services or national services such as alcoholics anonymous.
Only patients with suspected chronic liver disease should be referred to hepatology (see Alcohol related liver disease).
Services available:
Alcohol Concern www.alcoholconcern.org.uk
Useful information and publication section as well as “factsheets” that could be given directly to patients.
Drinkline Tel 0800 917 8282 (Available: 24 hours 7 days a week) or www.alcoholconcern.org.uk
Alcoholics Anonymous Tel 0845 769 7555 (7 days a week 10am –10pm) or www.alcoholics-anonymous.org.uk
Drinkware Trust Tel 020 7766 9900 (Available: 24 hours 7 days a week) or www.drinkaware.co.uk
Change Grow Live:
CGL Coventry
CGL, 1a Lamb Street, Coventry, CV1 4AE Tel 02476 010241 (Mon – Fri 9:00–5:00 and late opening Tues 9:00–8:00) or www.changegrowlive.org/coventry
CGL Warwickshire
CGL, 16 Court St, Leamington Spa, Warwickshire, CV31 2BB Tel 01926 353513 (Mon – Fri 9:00– 5:00) or https://www.changegrowlive.org/content/change-grow-live-warwickshire
Alcohol Related Liver Disease
Pre-referral investigations: FBC, LFT, GGT, ultra-sound abdomen
Referral threshold: Refer if there is evidence of cirrhosis (clinically or on ultrasound scan) or any evidence of hepatic decompensation (jaundice, ascites), otherwise continue surveillance in primary care, perhaps with LFTs every three months.
Encourage engagement with community alcohol services. Jaundice in the context of alcohol dependency requires urgent management including alcohol detoxification; consider admission to hospital. Severe alcoholic hepatitis carries a 50% 30-day mortality.
Ascites
Ascites has many causes and a first presentation requires urgent investigation.
The referral path will depend on the suspected aetiology. If chronic liver disease is suspected, please refer urgently to the hepatology clinic.
Elective admission for paracentesis can be arranged for patients with chronic liver disease who are known to the gastroenterology team. Please contact the hepatology secretary on 02476 966089 or the hepatology specialist nurses for advice 02476 967123, (safe haven fax 024 7696 6090)
Fatty Liver, Non-Alcoholic Fatty Liver Disease (NAFLD) or Non-Alcoholic Steatohepatitis (NASH)
See also: Non-Alcoholic Fatty Liver Disease (NAFLD) & Non-Alcoholic Steatohepatitis (NASH)
Gilbert’s Syndrome
In Gilbert’s syndrome, the bilbirubin is raised in isolation and is unconjugated. Request “split bilirubin” for confirmation. No need to refer unless there is diagnostic uncertainty. Exclude haemolytic anaemia.
Haemachromatosis
If you suspect haemochromatosis, please check transferrin saturation and HFE genotype. A raised ferritin can also be a secondary phenomenon (acute inflammatory response, fatty liver, alcohol excess, chronic liver disease), particularly if transferrin saturation is low.
Pre-referral investigations: LFT, ferritin, transferrin saturation, HFE genotype, ultrasound abdomen
Referral threshold: Suspected cases should be referred to haematology for venesection.
Patients who require hepatology input will be internally referred.
Consider screening family members (siblings).
Jaundice
Jaundiced patients with suspected biliary obstruction can be referred via the upper GI 2WW pathway. These patients will be offered an appointment in our rapid access jaundice clinic.
Patients with jaundice secondary to an acute hepatitic process can also be referred directly to the Jaundice Clinic, tel: 02476 967123
Patients with jaundice who have suspected decompensated alcohol related liver disease are likely to require hospital admission.
Please contact our hepatology nurse specialists (02476 967123), or the on-call gastroenterology SpR (bleep 4314) or consultant if in doubt, for further advice.
A rise in bilirubin with otherwise normal liver enzymes (isolated hyperbilirubinaemia i.e. Gilbert’s syndrome) does not require referral.
Liver Screen
A liver screen comprises tests for viral hepatitis, together with tests for genetic, autoimmune and metabolic abnormalities. The tests are outlined below:
- Viral hepatitis B and C serology (In acute hepatitis, also include hepatitis A, E, CMV and EBV)
- Immunoglobulins
- Liver antibodies (ANA, SMA, AMA-M2)
- Ferritin (If elevated, check transferrin saturation)
- Alpha-I-Antitrypsin levels (if low, need to check genotype – only need to refer homozygous individuals)
- Caeruloplasmin (only if patient under 40)
- Fasting glucose/lipids/HBA1C
Viral Hepatitis
Hepatitis B
All patients who are identified as chronic Hepatitis B carriers (Hepatitis B sAg positive) require assessment and follow up in secondary care regardless of liver function tests.
They are at risk of cirrhosis and hepatocellular carcinoma.
Please screen and vaccinate family members (household contacts).
Pre-referral investigations: HBV DNA, HBV eAg/ab, HIV, HCV, LFTs, clotting, AFP, Liver USS
Referral threshold: Refer all patients with chronic hepatitis B to hepatology via choose and book. The hepatology team triage the referrals and divert some patients to the infectious diseases (ID) team to reduce waiting times.
Hepatitis C
A positive hepatitis C antibody may reflect previous exposure to hepatitis C infection, rather than active viraemia.
Check HCV RNA. If RNA is positive, refer to the hepatology clinic, for anti-viral treatment.
If RNA is negative (often reported as <12), repeat the test at 3 months for confirmation.
If still negative, the patient can be reassured they do not have Hepatitis C infection.
Highly effective, oral drugs are now available to treat hepatitis C with cure rates of 96-100%. All RNA positive patients should be offered treatment.
We also run assessment and treatment clinics at the community drug team in Coventry (CGL), to treat patients receiving methadone treatment who may struggle to attend hospital appointments.
Pre-referral investigations: HCV RNA, LFT, HBV serology, HIV
Referral threshold: Refer all HCV RNA positive patients
Hepatitis A & E
Hepatitis A and E viruses are transmitted via the faeco-oral route.
They cause an acute self-limiting illness in the vast majority of cases. Rarely, patients may develop fulminant hepatitis (manifest by rising INR). These infections are notifiable to public health.
If there is clinical concern, patients can be referred to the rapid access jaundice clinic or discussed with the on call gastroenterology SpR (9-5pm).
Wilson’s Disease
Rare genetic disorder, diagnosis extremely unlikely over the age of 40.
Pre-referral investigations: for suspected cases, check ceruloplasmin, LFTs and ultrasound abdomen
Referral threshold: refer all suspected cases
Leave feedback
You must be logged in to post a comment.