Acute Kidney Injury
AKI is a clinical and biochemical syndrome reflecting abrupt kidney dysfunction
AKI stage is determined by acute changes to serum creatinine and / or urine output
AKI usually occurs secondary to acute illness ( commonly sepsis) Identifying underlying acute illness causing AKI is key to establishing primary diagnosis
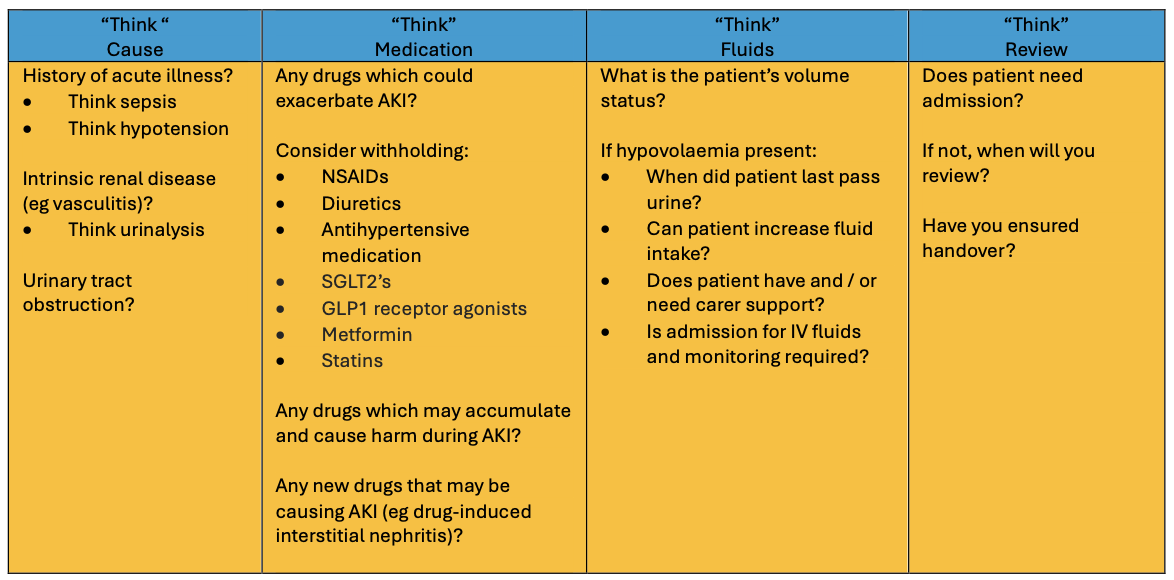
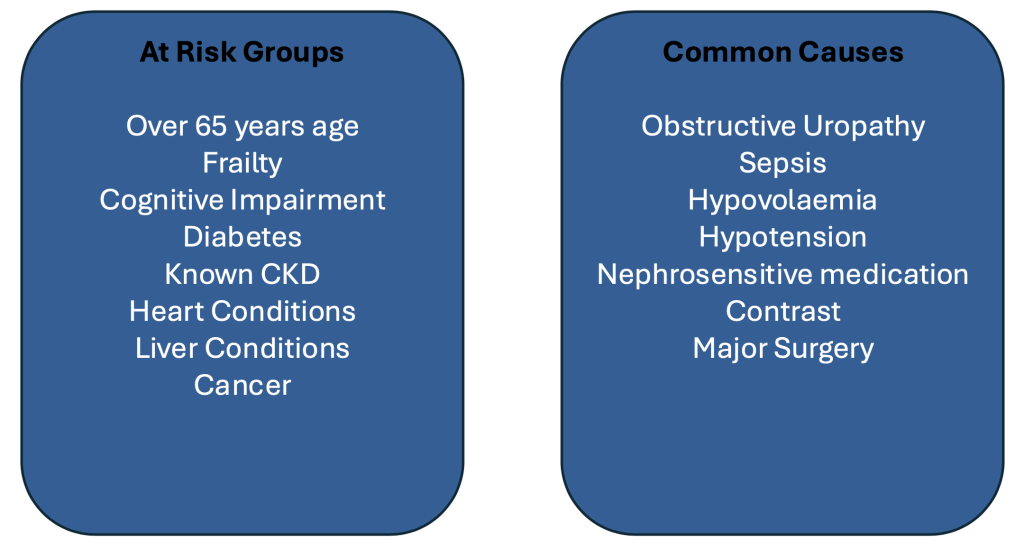
Key tables below
Full versions in RCGP AKI thumbnail link below (and link right)

Click on image below to access “Think Kidneys” Website with patient and primary resources

Acute Kidney Injury (AKI) in the Community
AKI – a rapid reduction in kidney function resulting in a failure to maintain fluid, electrolyte and acid-base homoeostasis. Approximately 65% of AKI starts in the community
Definition of AKI – Kidney Disease: Improving Global Outcomes (KDIGO)

Background of Acute Kidney Injury AKI
The NHS is the first health system in the world to attempt to tackle AKI with a system-wide approach.
- Up to 100,000 deaths each year in hospital are associated with AKI
- Up to 30% of those deaths could be prevented with the right treatment and care
- 1 in 5 people admitted to hospital as an emergency has AKI
- Around 65% of AKI starts in the community
- 15 million people in the UK live with long term conditions which are more prevalent in older people placing them at greater risk of AKI
- The annual cost of AKI-related inpatient care in England is estimated at £1 billion, just over 1% of the NHS budget
Distinguishing AKI and CKD
- Most patients with Acute Kidney Injury (AKI) look unwell, may have hyperkalaemia (potassium > 6.0 mmol/L), and usually need admission or rapid review according to the guidance above
- Patients with CKD usually look well, and may have other complications of CKD (eg anaemia, low calcium, high PTH etc)
- If hyperkalaemic, they may also need admission or rapid review. AKI on CKD exists and can have a mixture of all these features, and should be managed as AKI
AKI Prevention in Primary Care – Medicines Sick Day Card (Healthcare Improvement Scotland)
The primary aim is prevention of AKI through education of the patients (making them aware of their higher risk), regular medicines management reviews and sick day guidance
Use the Sick Day Card for vulnerable patients (especially the elderly, with polypharmacy, and CKD)
This asks the patient to stop a range of drugs including Metformin, ACE/ARB, NSAIDs and diuretics for a few days if they are feeling unwell (especially septic, eg fever, gastroenteritis, UTI).
The will probably need to restart them 24-48 hours later, when better, and eating and drinking normally or consult their GP if unsure
Follow link for a copy of the card

Click on image below for link to full RCGP Toolkit

Useful links:
Think Kidneys Quick Reference Guide
Think Kidneys Recognising and Responding to Acute Kidney Injury for Adults in Primary Care Table
GP Gateway Electrolyte Abnormalities
Think Kidneys Primary Care Advice for Medication Review in AKI Quick Guide to problematic drugs
Think Kidneys Restarting ACEI ARB Diuretics Antihypertensive drugs after AKI Restarting Medications
Think Kidneys Sick-Day Guidance 2018
Patient Information
Think Kidneys Patient Infographic
Think Kidneys Patient at Risk Leaflet_Printout
Care Home Information & Guidance
Think Kidneys Care Homes Resources
Think Kidneys Could my patient have Acute Kidney Injury?
UHCW Acute Kidney Injury (AKI) Service
Dr Krishna Appunu – Consultant Nephrologist – Bleep 4474
Rachael Lee – Advanced Nurse Practitioner & Lead Nurse – Bleep 5009
Esther Theophilus – Nurse Practioner – Bleep 5233
Outlier Registrar – Bleep 4134
Provides clinical review of in-patients at UHCW that flag via the CRRS alert system as having an AKI 1, 2 or 3 and work closely with the parent teams to identify cause of AKI and an appropriate management plan to treat and resolve the AKI
AKI Clinics
All patients that have been reviewed by either the Advanced Nurse Practitioner or Clinical Nurse Specialist during their inpatient stay that had either an AKI 2 or an AKI 3 will be invited to a post discharge clinic 2-3 weeks post discharge
Purpose of the clinic: to monitor the renal function to ensure AKI has resolved to baseline, organise any further investigations and to educate the patients about their AKI to aim to reduce or prevent further AKI’s for these patients
AKI Referrals
Patients that have an AKI 3 or are too sick to manage in primary care should be referred either via Accident & Emergency or through the GP liaison Team (02476 966223 or Bleep 1424)
Information to send with referral
- Medical History – including recent blood tests, urinalysis, MSU, ACR,PCR results
- Previous tests of renal function and dates
- Medications including recent prescriptions or alterations
- Examination findings and observations
- Imaging investigations & results i.e. CXR, USS KUB, Contrast procedures
- Recent surgery – dates & complications
Useful Links & Documents
Think Kidneys AKI Promotion Programme
Professional Resources
Follow link for additional professional AKI resources page
Leave feedback
You must be logged in to post a comment.