USC Referral Criteria for Skin Lesions
TELEDERMATOLOGY
In line with National mandate to implement teledermatology, patients referred on USC pathway who are appropriate for teledermatology will be offered image capture appointments
Where image capture appointments are limited, patients will continue to be offered a face-to-face appointment
Please ensure the referral form is completed fully including the clinical narrative and access needs/adjustments. This information is critical to allow appropriate appointments/locations to be booked for patients and avoid delay in their care
Please try to ensure the referral form is completed in the presence of the patient as some of the required information would not be routinely asked
Alongside the referral form, an FAQ referral document is available.
Patients will be able to access further information about teledermatology online @ Happy Healthy Lives
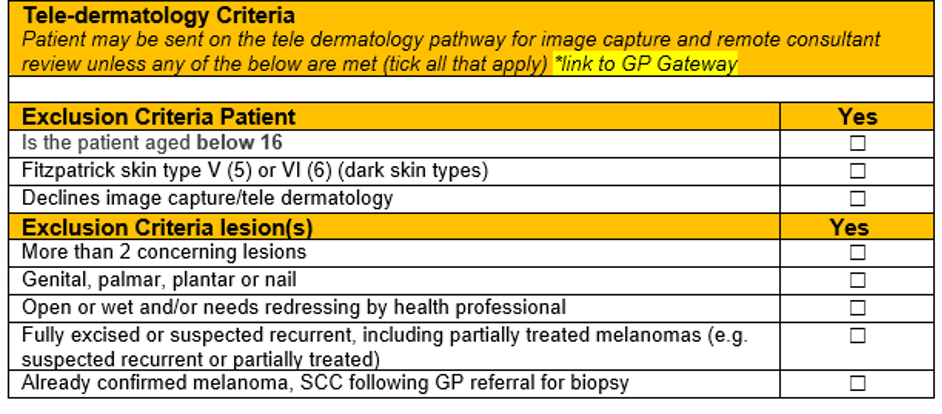
It is recognised that lesions may be more challenging to assess and diagnose in patients with brown or black skin when assessed using images. As such, patients with skin types 5 or 6 (Fitzpatrick scale) will follow a face-to-face pathway and are excluded from the teledermatology pathway
Skin of Colour – BAD Patient Hub (skinhealthinfo.org.uk)

MELANOMA
Clinicians may use EITHER the ABCD rules OR NICE weighted 7-point checklist:
A B C D rules apply to melanocytic lesions only. Change often occurs in 3-12 months
Melanomas are generally not keratotic (crusty), unlike Seborrhoeic Keratoses Please indicate if there has been any change in:
A. Asymmetry (change in symmetry)
B. Border (change to be irregular, blurred edges)
C. Colour (change in colour or change to have more than one colour, even if lighter)
D. Diameter (change in diameter, especially if change to be greater than 6mm)
OR: NICE weighted 7-point checklist score of 3 or more
MAJOR features of the lesions (scoring 2 points each):
- Change in size
- Irregular shape
- Irregular colour
MINOR features of the lesions (scoring 1 point each):
- Largest diameter 7 mm or more
- Inflammation
- Oozing
- Change in sensation
Additional important clinical information
- Previous history of skin cancer
- Family history of skin cancer
- Immunosuppression
- Pacemaker (or another electronic implanted device?)
- Please include the history and location of the lesion and attach any photographs.
SQUAMOUS CELL CARCINOMA (SCC)
These are from Keratinocytes and usually have adherent keratin. Poorly differentiated SCCs can just be ulcerated. Refer Keratoacanthomas as if they are SCCs.
NB: Usually appear as a red, prominent nodule or a non-healing ulcer. In some cases, a keratin core is present (possible keratoacanthoma) which should be referred in case they are SCCs.
Features:
- Dermal induration (nodular)
- Expansion over weeks to months
- Tender
- Keratin producing (adherent)
- Ulcerated pink lesion
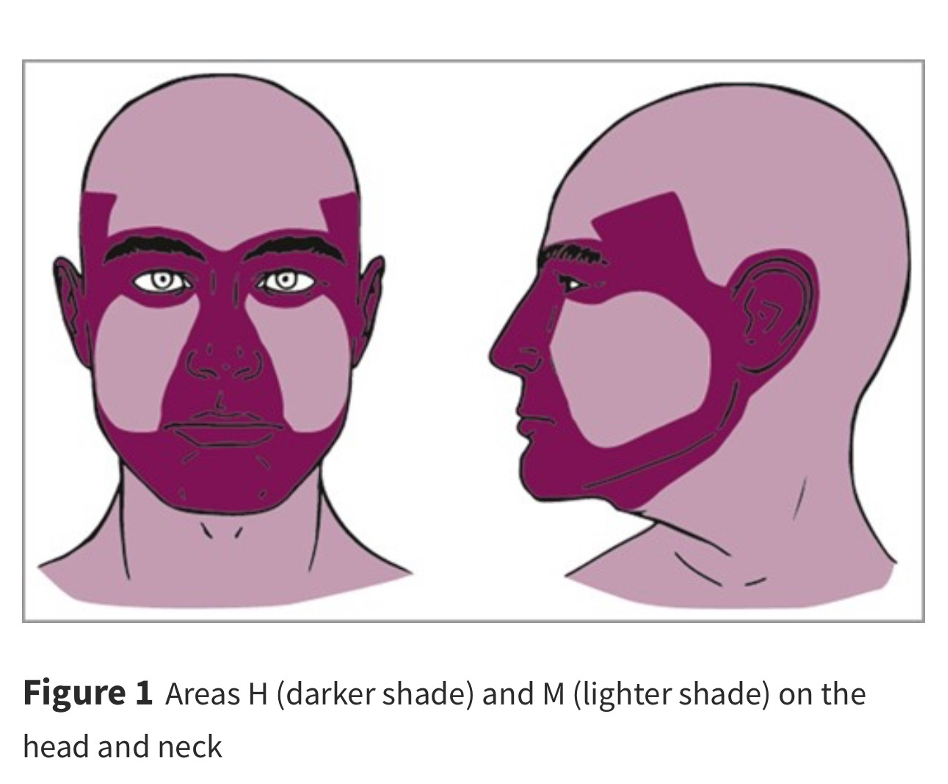
CRITICAL SITE BASAL CELL CARCINOMA (BCC)
Critical sites:
Critical Site BCC’s are located in the darker shaded areas H
(If <2 cm and not critical site refer routinely to community dermatology providers)
Additional important clinical information:
- Previous history of skin cancer
- Family history of skin cancer
- Immunosuppression
- Anticoagulants
- Pacemaker (or another electronic implanted device)
Please provide the patient a Cancer Research UK Information Sheet – follow link
Leave feedback
You must be logged in to post a comment.