C&W Guide for GPs: Unscheduled Bleeding on HRT
Purpose of this guidance
The purpose of this guidance is to provide recommendations for the safe and appropriate management of women experiencing unexpected bleeding on hormone replacement therapy who present to primary care physicians
It has been written with the aim of avoiding unnecessary investigation of women at low risk of endometrial cancer who experience bleeding within six months of initiating HRT or within three months of a change in dose or preparation in those already established on HRT
It is anticipated that the introduction of these guidelines will allow women at increased risk of endometrial cancer to be prioritised for investigation, avoiding unwanted cessation of HRT and anxiety for those at low risk
The majority of patients should be suitable for management outside of Urgent Suspected Cancer pathways (USCP)
This guidance has been written with reference to the British Menopause Society/British Gynaecological Cancer Society guidance published in April 2024: Management of unscheduled bleeding on hormone replacement therapy (HRT) – British Menopause Society (thebms.org.uk)
Definitions
- Unexpected/unscheduled vaginal bleeding: Bleeding which occurs outside of the scheduled withdrawal bleed in women taking sequential HRT (sHRT)
- Bleeding at any time in women using continuous combined HRT (ccHRT)
N.B. Unscheduled bleeding is NOT the same as post-menopausal bleeding, the definition of which is bleeding after > 12 months of amenorrhoea in women NOT on HRT
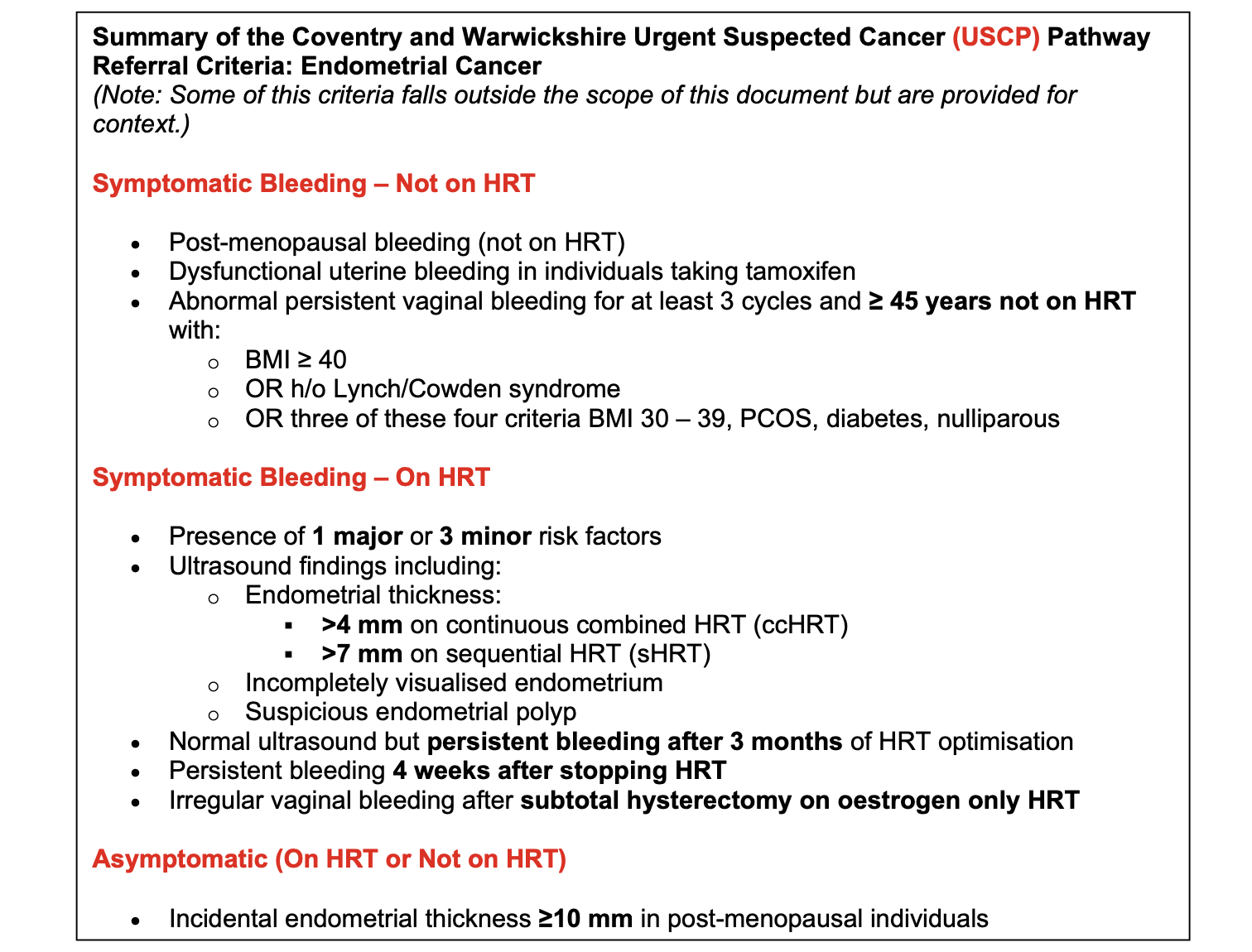
Women who meet the definition of post-menopausal bleeding should be referred on USCP
Background
Endometrial cancer is the fourth most common cancer in women
Abnormal uterine bleeding (AUB) is the most common presenting symptom of endometrial cancer, however, less than 5% of peri and post-menopausal women who present with this symptom in the UK each year have endometrial cancer (Clarke et al. 2017)
Over the last ten years prescriptions of hormone replacement therapy HRT in peri-menopausal and menopausal women have increased, consequently increasing the numbers of women presenting with unscheduled bleeding
Unscheduled bleeding is common within the first six months of initiating HRT, and also within three months of a change in dose or preparation in those already established on HRT
It can affect up to 38% of people using sequential HRT and 41% using continuous combined HRT
-
Understanding the risks of Endometrial Cancer (EC) with HRT:
Women taking ccHRT without bleeding are thought to be at lower risk of Endometrial Cancer than those not on HRT
Women on sHRT (standard dose oestrogen with appropriate progesterone opposition) after age 50 without unscheduled bleeding used for less than 5 years are thought to be at the same risk as those not taking HRT
Cancer risk increases in women using sHRT with insufficient progesterone (either not in proportion to the oestrogen dose or not taking it for long enough each month), sHRT >5 years, tricyling with progestogen every 3 months >1 year, unopposed oestrogen
Risk of EC with ABNORMAL bleeding:
PMB without HRT: Approximately 10% of women who experience PMB and are not on HRT will be diagnosed with EC
Those women with unscheduled bleeding on HRT have a 1-2% risk, however unscheduled bleeding with a thickened endometrial increases the risk of EC including hyperplasia to 1.3-5%
Initial Assessment
The aim of the initial assessment in primary care is to assess risk factors for endometrial pathology as well as optimise usage of HRT
Important points to note in the history:
- Bleeding pattern and any precipitating factors
- Any associated symptoms, e.g pain, discharge, urinary symptoms
- HRT
- Preparation
- Dose
- Duration since initiation or change in preparation
- Compliance
- Smear history
- Sexual history and risk of infection
- Pregnancy risk
- Are they on any GLP-1 agonist?
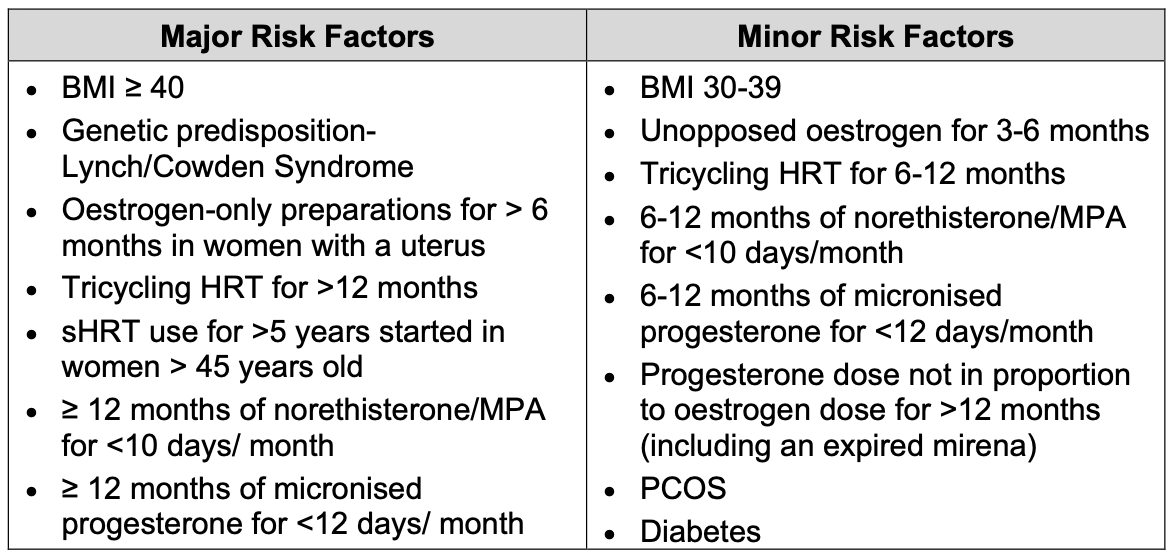
Risk factors for endometrial cancer
Important points on examination:
Ruling out other differentials is essential. If the patient declines examination, please document this clearly in any onward referral
- Evidence of an ovarian mass
- Vulvovaginal atrophy, ulceration or prolapse
- Cervical appearance
- Pregnancy test if appropriate
- BMI
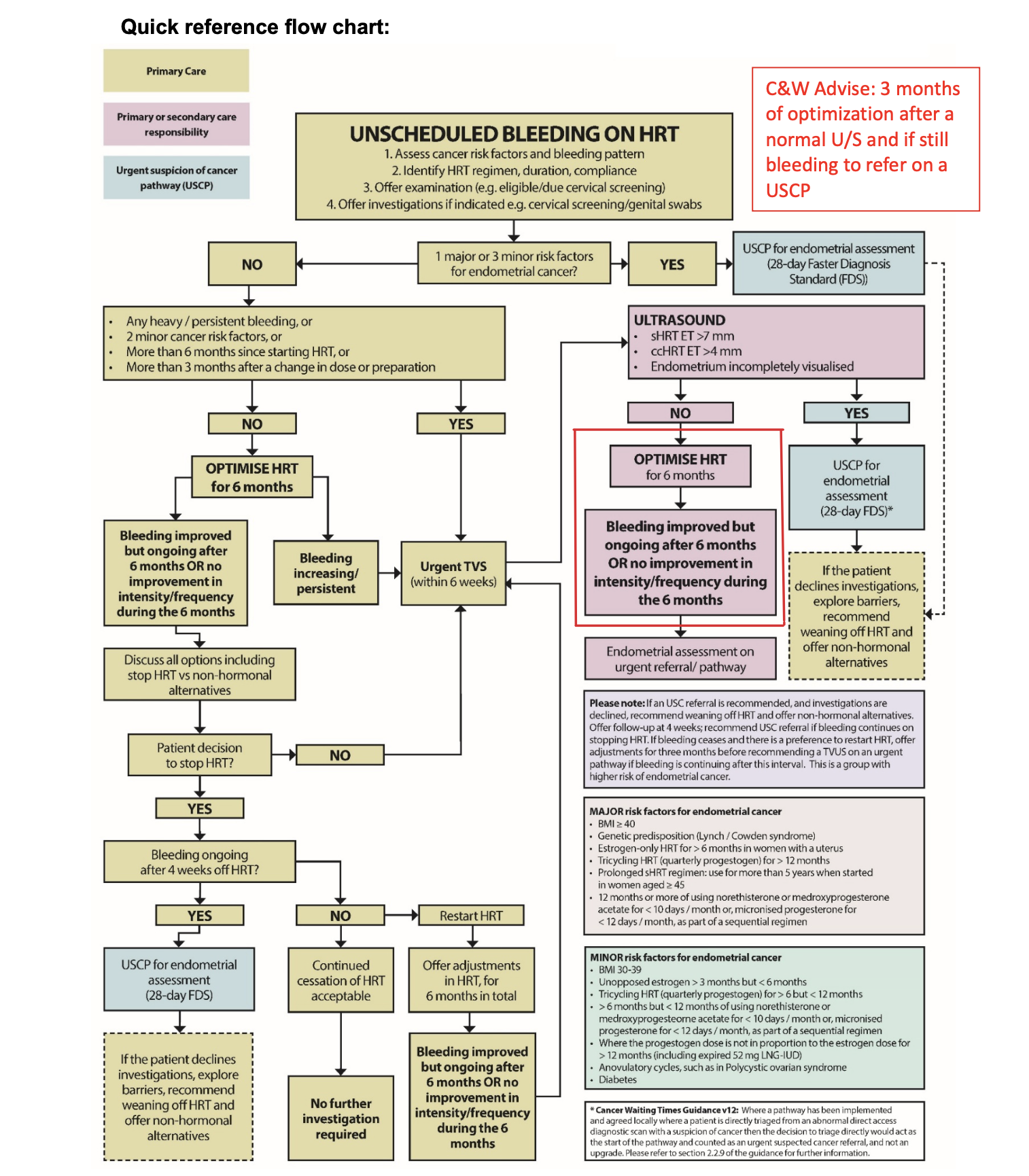
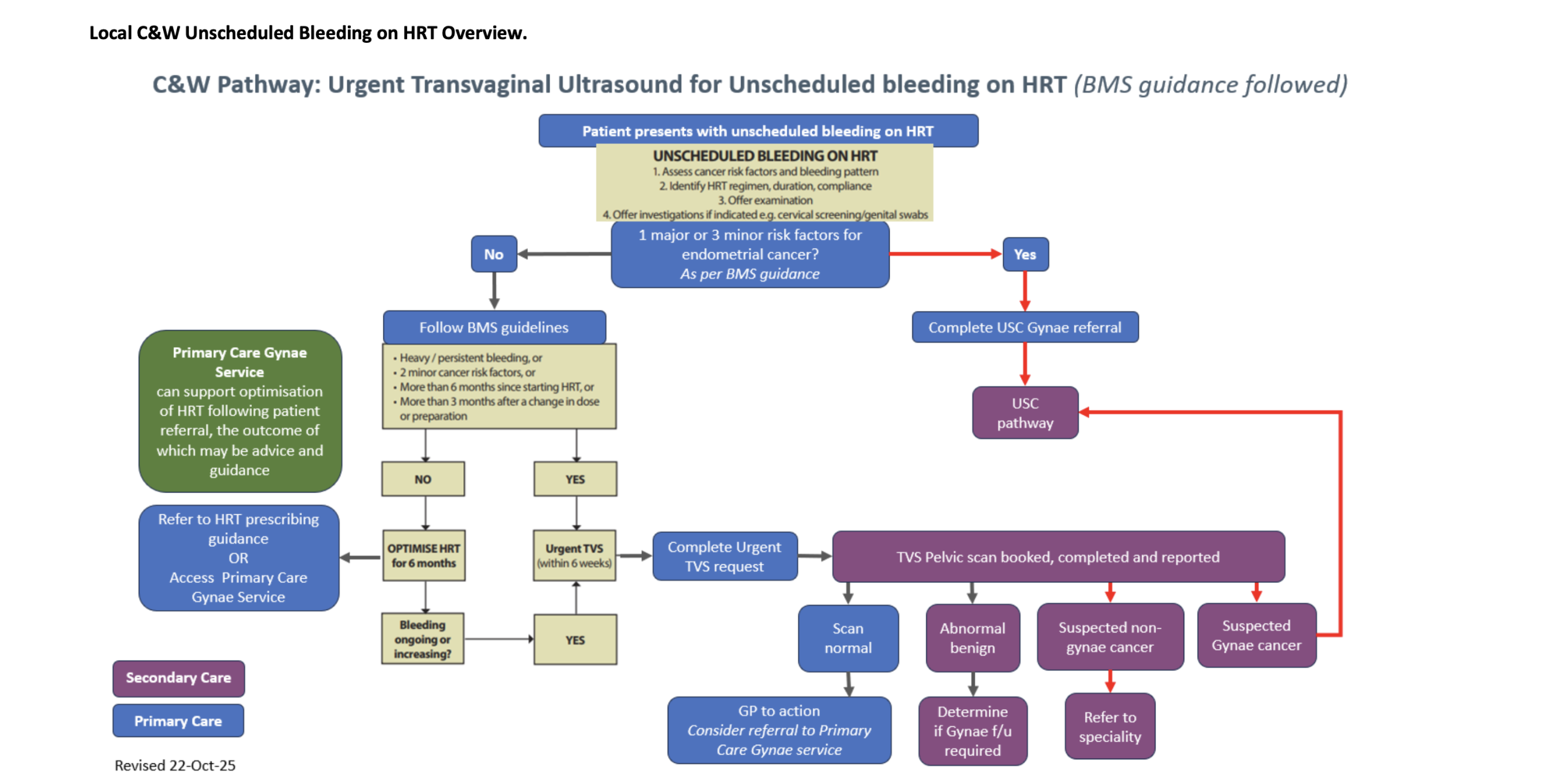
When to investigate unscheduled bleeding on HRT
If there are no individual risk factors (1 major or 3 minor risk factors) or any indication to do urgent pelvic ultrasound scan offer HRT/ progesterone adjustments for a total of 6 months
If symptoms persist > 6 months after initiating HRT or > 3 months of changing HRT and compliance is good then assessment and investigation is indicated
High Risk:
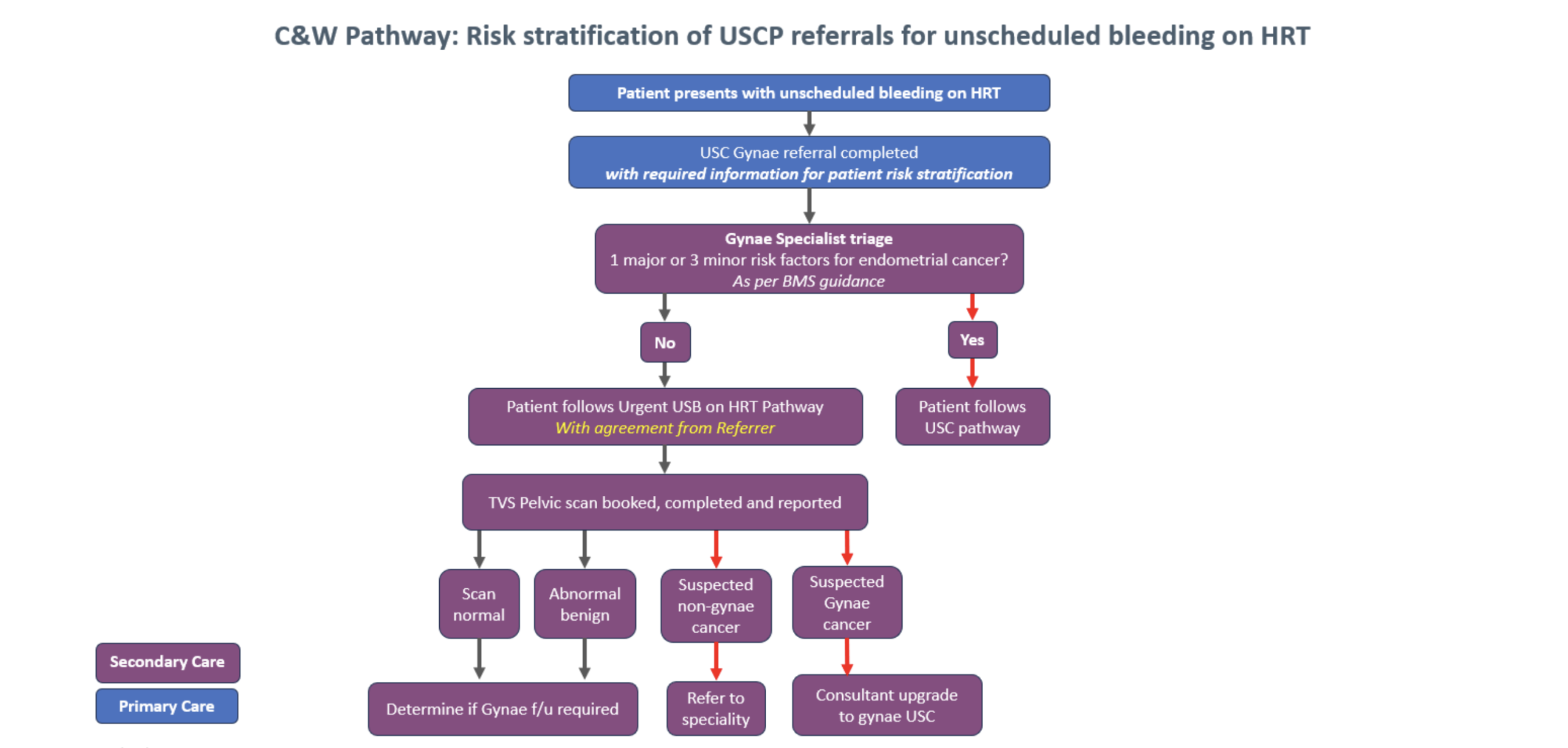
Women regarded as at increased risk for endometrial cancer with one major or three minor risk factors, presenting with unscheduled bleeding on HRT should be referred on the USCP
Medium/ Low risk:
If unscheduled bleeding occurs in women in the following situations they should be assessed to exclude endometrial pathology with an urgent pelvic ultrasound scan:
- More than six months after starting HRT or
- After three months following a change in HRT dose or preparation or
- Where women have two minor risk factors irrespective of the interval since starting HRT or
- Prolonged / heavy bleeding* on HRT irrespective of the interval since starting HRT
*Defined as: Prolonged withdrawal bleeds (more than 7 days), and / or — Heavy bleeding (flooding and / or clots), and / or — Persistent bleeding, even light, which occurs most days for 4 weeks or more
What to do with the results:
- If the scan is abnormal: Defined as: ET: > 4 mm for ccHRT or > 7 mm for sHRT or endometrium incompletely visualized / suspicious polyp.
Patients will be offered onward referral on an USCP for endometrial assessment (biopsy and / or hysteroscopy) by the Trust
As long as the appropriate referral pathway has been followed using the new urgent TVS request form, this will be dealt with by Secondary Care
- A thickened endometrium found on scan by any other provider would then need referral on the USCP form
- If the scan is normal: Women with unscheduled bleeding, in the presence of a uniform endometrium (normal scan) which is fully visualised, and measures ≤ 4 mm with ccHRT or ≤ 7 mm with sHRT, can be reassured that the risk of endometrial cancer is low
Offer HRT adjustments if feel confident to do so for 3 months and then offer endometrial assessment, on an USCP, if bleeding increases during the 3 months or, is continuing after this interval
Adjustments can either be made by the GP or by referral to the PCGS. Please see section 9.
Adjusting/optimising HRT to reduce unscheduled bleeding episodes
01-BMS-GUIDELINE-Management-of-unscheduled-bleeding-HRT-NOVEMBER2024-A.pdf (Table 6)
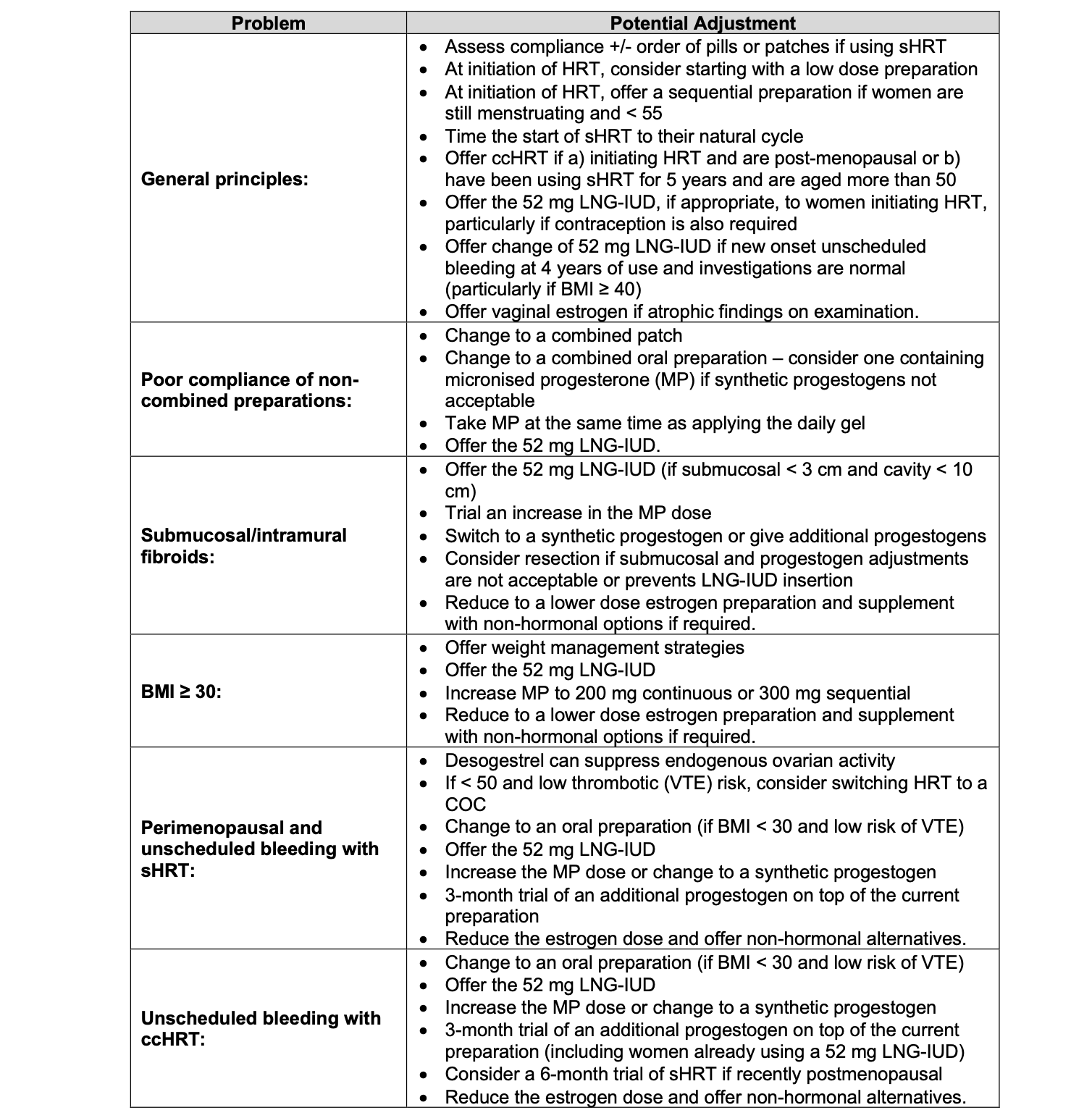
Oestrogen doses and proportional progesterone doses
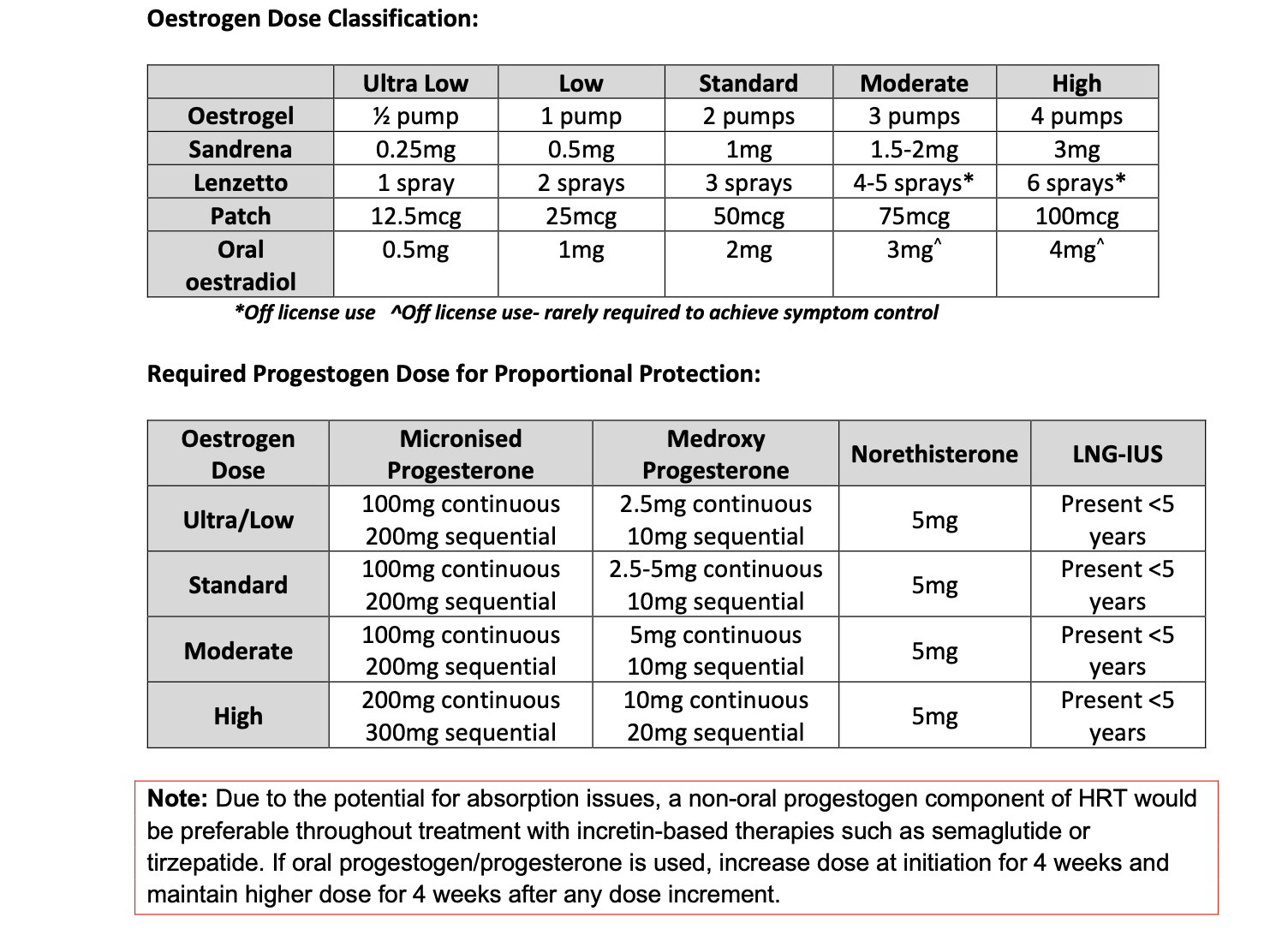
Nalvee (Dydrogesterone):
Sequential regime: 10 mg dydrogesterone during the last 14 days of each 28-day cycle.
Depending on the clinical response, the dosage may be adjusted to 20 mg dydrogesterone daily in the course of the treatment.
For further information regarding the management of menopause, please refer to CG051 Management of Menopause Guidelines Nov 25
Ten Practical Tips for HRT Prescribing and Troubleshooting for GPs
- Any women NOT on HRT presenting with post menopausal bleeding should be referred on the USCP.
- For those with bleeding on HRT (< 6 months) in the absence of risk factors, consider changing or altering progesterone dose.
- Ensure patients with a 52mg levonorgestrel releasing intrauterine system (IUS) (eg. Mirena, Benilexa and Levosert) used for HRT have recalls in place to ensure expiry date is clearly recorded. Ref: BNF Menopause: HRT
- Ensure dose of oestrogen is properly recorded on notes – specify number of pumps of transdermal gels/sprays on prescription.
- Have a robust HRT review process in practice, check patients are taking their HRT correctly. Ask about bleeding, check type of HRT is appropriate for age and risk factors, check progesterone regime is adequate/IUS in date for women with uterus. Offer health promotion where applicable – cervical screening/breast screening etc.
- Consider running a search for women on high dose oestrogen (with a uterus) and ensure they have adequate progesterone protection (see dosing tables) .
- Consider running a search for women taking sequential (sHRT) over the age of 45 – they should be offered, after five years of use or by age 54 (whichever comes first), a change to continuous combined (ccHRT).
- Know your risk factors for endometrial cancer – consider these in women presenting with bleeding on HRT as may need urgent referral.
- Know your local pathways for requesting a direct access transvaginal ultrasound.
- Keep the BMS guidelines and BMS tools for clinicians in your bookmarks for reference
References:
British Menopause Society/British Gynaecological Cancer Society guidance published in April 2024: Management of unscheduled bleeding on hormone replacement therapy (HRT) – British Menopause Society (thebms.org.uk)
The prevalence of endometrial cancer in women with postmenopausal bleeding: a systematic review and meta-analysis (Clarke et al. 2017)
DISCLAIMER
Efforts are made to ensure the accuracy and agreement of these guidelines, including any content uploaded, referred to or linked to from the system. However, Coventry and Warwickshire ICB cannot guarantee this. This guidance does not override the individual responsibility of healthcare professionals to make decisions appropriate to the circumstances of the individual patient, in consultation with the patient and/or guardian or carer, in accordance with the mental capacity act, and informed by the summary of product characteristics of any drugs they are considering. Practitioners are required to perform their duties in accordance with the law and their regulators and nothing in this guidance should be interpreted in a way that would be inconsistent with compliance with those duties
Information provided through GP Gateway is continually updated so please be aware any printed copies may quickly become out of date.
Local C&W Unscheduled Bleeding on HRT Overview
Example cases
A 49-year-old lady with diabetes and BMI 31 and on sHRT has noticed some unscheduled bleeding after 2 months of starting it Answer: History and examination; 2 minor risk factors so urgent u/s scan
A 52-year-old lady on ccHRT met the criteria for an urgent Pelvic u/s for unscheduled bleeding and her ET was 5mm. Answer: Onward referral will be done by the Trust
A 50-year-old lady been on sHRT for 3 months and bleeding not settled, no risk factors, so progesterone modified. 3 months later still bleeding. Answer: History and examination and Urgent U/s scan: As bleeding for a total of 6 months and adjustments already made.
A 53 three old lady on ccHRT has had an u/s scan as there were concerns she may have fibroids. It shows she has an ET of 11mm? Answer: USCP referral
| Author: | Title | Date |
| Dr. Rebecca Jacques | GP and C&W ICB Women’s Health GP Lead, BMS Accredited Menopause Specialist. | 19/12/2025 |
| Reviewed by: | ||
| Dr. Hazel Blanchard | GP and C&W ICB Primary Care Clinical Cancer Lead | 19/12/2025 |
| Dr. Jill Crowfoot | C&W ICB Gynaecology Clinical Convenor, C&W Primary Care Gynae Service Clinical Lead | 19/12/2025 |
Leave feedback
You must be logged in to post a comment.