About the Paediatric Allergy Service
The members of the UHCW NHS Trust team include:
The Paediatric Allergy Service at UHCW
Members
- Dr Anjli Jethwa – Consultant Paediatrician with Allergy interest
- Dr Aled Picton – Locum Consultant Paediatrician with Allergy interest
Lead Health Professionals
- Sarah Pitts CNS Allergy lead
- Catherine (Kate) Weller CNS Allergy
- Paige Reed CNS Allergy
- Linda Cross CNS Allergy
- Paula Cassidy CNS Allergy
- Rachel Ball Paediatric Dietitian lead
- Nina Nichols Allergy Team admin
When To Refer To Allergy Clinic
- Anaphylaxis
- IgE Food Allergies
- FPIES (Food Protein-Induced Enterocolitis Syndrome)
- Chronic Spontaneous Urticaria/Angioedema
- Venom Allergy
- Allergic Rhinitis IF unresponsive to standard medical treatment
If in doubt use A&G
Allergy Focused History
See link on the right re: BMJ article on EATERS method to diagnose food allergies
Also need to include personal or family history of atopy
IgE Mediated
- Exposure – eating, or occasionally by skin contact, or rarely inhaled
- Allergen – milk, egg, peanut, tree nut, sesame seed most common
- Timing – symptoms occur within 1 hour of ingestion, during weaning or at first known exposure
- Environment – allergen is new part of diet
- Reproducible – always has symptoms with exposure, “gap” in regular consumption
- Symptoms:
- skin – urticaria, angioedema
- gut – vomiting and abdominal pain, diarrhoea
- respiratory – acute onset cough, wheeze, stridor, clear rhinorrhoea
- neurological – sleepiness, impending doom, anxiety
- cardiovascular – collapse, shock
Red flags – anaphylaxis
Non-IgE Mediated
- Exposure – cow’s milk formula fed, or breast fed with regular exposure through mother’s milk
- Allergen – milk and soya most common
- Timing – symptoms occur 1-24 hours after ingestion, in first year of life, onset can be insidious
- Environment – allergen is a regular part of the diet or of the mother’s diet if breast fed
- Reproducible – symptoms may take time to settle on an exclusion diet, 2-14 days, symptoms return on reintroduction of allergen within 6 weeks
- Symptoms:
- skin – eczema
- gut – vomiting, reflux, dysphagia, food bolus impaction, colic, abdominal pain, diarrhoea or constipation, mucous/blood in stools
- respiratory – chronic catarrh, cough, persistent clear rhinorrhoea
Red flags – vomiting and diarrhoea leading to shock (FPIES); faltering growth
Allergy Tests
IgE Food Allergy – focused testing base on history:
- Serum IgE
- Skin Prick Test
Non-IgE Food Allergy – No blood test needed
Unrecognised allergy tests:
- vega testing
- applied kinesiology
- hair analysis
- serum-specific IgG testing
Prognosis of Food Allergies
- Most children will outgrow milk, egg, soya allergies by school age- may tolerate baked forms and progress along ladders
- Other food allergies tend to be lifelong
- 20% of children can outgrow nut allergy
- Ongoing management to support Health Transition:
- Practical Ps for Allergy Patient (BSACI) – https://www.bsaci.org/about-bsaci/bsaci-council-and-executive/bsaci-subcommittees/adolescents-and-young-adults-resources-practical-ps/
- Ready Steady Go website
- www.11to25hub.com
Pollen Food Allergy (PFS)* new BSACI guideline content

Pollen food syndrome (PFS) is a common, IgE- mediated food allergy, characterised by immediate mild oro-pharyngeal symptoms after the consumption of raw plant foods due to ross reactions between pollen antibodies and unstable plant food allergens.
- Main pollens involved in the UK are tree pollens, principally birch tree pollen, hazel and alder.
- Usually affects adolescents or adults, but can occur in children of any age, especially those who suffer from spring or summertime hay fever.
- The diagnosis and management of PFS can often be wholly managed in Primary Care but differentiating between PFS and an allergy to tree nuts/peanuts can be difficult, so reactions to the latter usually require onward referral to Secondary Care.
Clinical History
Clinical history alone can be diagnostic. The history taking should include questions regarding:
- Reported symptoms – PFS is characterised by mild immediate itching and/or swelling of the oropharynx, which responds to antihistamine but may resolve without any treatment
- Food triggers – PFS involves symptoms only to raw (uncooked) plant foods, with cooked or processed foods usually tolerated.
The most common food triggers include:
- apples, cherries, plums, peaches, kiwifruit, pear, carrot, celery, or tomato
- hazelnuts, almonds, walnuts, or peanuts
- soya milk, soya protein powder or edamame beans
- peeling potatoes or other root vegetables – causes itchy hands
History of allergic rhinitis – PFS is most common in people reporting hay fever in springtime, but often also experience symptoms in the summer or autumn.
Management
No need for allergy tests or onward referral to secondary care if symptom history and food triggers are consistent with PFS, and reactions are only to fruits or vegetables.
- Advise to avoid only those raw foods which have already provoked symptoms
- Provide with patient information leaflets on PFS
- Refer to a community dietitian if many fruits or vegetables trigger reactions, or the diet is already compromised due to other dietary restrictions
- Treat optimally for co-morbidities such as rhinitis, asthma and eczema.
When to Refer to a Secondary Care Allergy service
- Those reporting any symptoms to:
- Tree nuts
- Peanuts whether mild, moderate or severe
- Soya milk and/or raw/cooked fruits/vegetables (systemic or severe reactions)
- Use Advice and Guidance service if uncertainty whether reported symptoms merit referral, or if any specific blood tests should be undertaken,
When making a referral please consider the following:
- Providing details on triggers, symptom type, time to onset and whether triggers include both cooked and raw foods will help the specialist allergy service risk assess the patient
- Those reporting severe reactions, especially if they also have asthma, will need to be prescribed adrenaline auto-injectors (AAI), and trained to understand how and when to use them, so that they are safety netted prior to being seen in secondary care
- Most people with PFS do not need AAI, so the continued need for an adrenaline autoinjector will be reassessed by the Allergy Service following the referral
- Once the referral has been accepted, the patient should be advised that they will be contacted by the allergy service regarding any instructions preparatory to allergy testing, such as discontinuation of antihistamine.
Patient information leaflet
Click on image below or link on right

Approach to Urticaria
Chronic Spontaneous Urticaria:
- Daily symptoms for 6 weeks or more
- Can be associated with angioedema
- CRUSE app https://ucare-network.com/cruse-chronic-urticaria-self-evaluation-app/
- 25% are disease free after 3 years, 90% after 7 years
- Most respond to non-sedating antihistamines
- Investigations: FBC, ferritin, TFTs, antithyroid antibodies, LFTs, coeliac screen, urinalysis (C3/C4 only if urticaria is not pruritic)
- Management: daily non-sedating antihistamines, dose can be doubled (x4 dose under specialist supervision); consider montelukast (informed decision, BNFc product information leaflet)
Acute intermittent – history all important:
- Physical (cold, pressure)
- Viral illnesses
- Food triggers
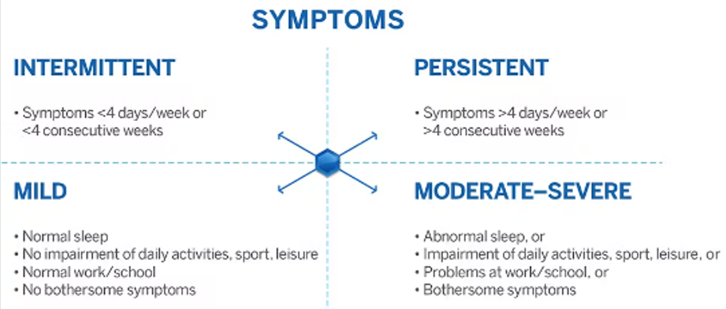
Rhinitis
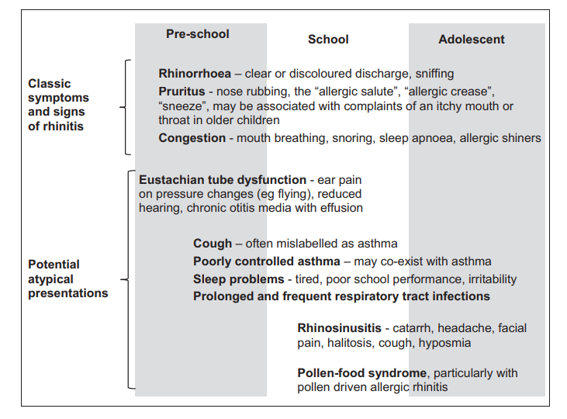
Examination:
- General assessment (including growth parameter, systemic examination)
- Allergic salute/horizontal nasal crease, chronic mouth breathing, allergic shiners
- RED FLAGS: depressed or widened nasal bridge, purple nasal tip
- Anterior rhinoscopy
- Pale, hypertrophied nasal turbinates, secretions, septum position, throat examination
- RED FLAGS: polyps, crusting
Causes are generally allergic, non-allergic or infective
Non allergic causes:
- Non-allergic rhinitis with eosinophilia
- Autonomic/vasomotor
- Drugs (beta blockers, chlorpromazine, cocaine, nasal decongestants, NSAIDs)
- Hormonal
- Food (alcohol, spicy foods, peppers)
- Atrophic
- CF, Primary Ciliary Dyskinesia
- Systemic/inflammatory
- Immunodeficiency
Management:
- Nasal washing (Cochrane Database Syst Rev. 2018 Jun 22;6(6):CD012597.)
- Non-sedating oral antihistamines (cetirizine, loratadine, desloratadine, fexofenadine)
- Topical nasal steroid sprays (Nasonex, Avamys, Dymista, Ryaltris)
- Antihistamine eye drops (olopatadine, sodium cromoglycate)
- Leukotriene receptor antagonists (montelukast)
Nasal steroids licensing:
- Nasonex – mometasone (>3 yo)
- Avamys – fluticasone (>4 yo)
- Dymista – fluticasone and azelastine (>12 yo)
- Ryaltris – mometasone and olopatadine (>12 yo)
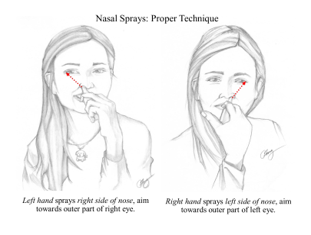
- Correct administration (https://www.itchysneezywheezy.co.uk/)
Referral to ENT:
- Unilateral symptoms
- Blood-stained discharge
- Pain
- Structural abnormalities e.g. septal deviation
Referral to Allergy Clinic:
- Treatment for children with the persistence of symptoms despite appropriate medications
- Immunotherapy an option, as is Grazax/Acarizax
Drug Allergy in Children (Suspected Antibiotic Allergy only)* restricted service available
Guidance regarding referral advice for the Paediatric Allergy Service should be read in conjunction with NICE CG183 Diagnosis and Management of drug allergy www.nice.org.uk/guidance/cg183
Drug Allergy Assessment
- Immediate reactions usually occur <1hour after drug exposure
- Non–Immediate reactions occur within a few days or weeks
See Nice.org.uk CG183 pages 10-11 for distinguishing features www.nice.org.uk/guidance/cg183
Inclusion Criteria
- Anaphylaxis
- Severe non-immediate cutaneous reactions eg Stevens Johnson Syndrome
- If in case of presumed beta lactam and or cephalosporin / cephalosporin allergy a specific condition can only be treated by a beta lactam
- If there is likely to be recurrent requirement for that drug in the future eg beta lactam allergy in patient with immunodeficiency
- Allergy to more than one class of antibiotic
If the reaction was an immediate type please refer to the Paediatric allergy team and whilst waiting for the appointment please give the following advice:
Complete avoidance of the allergen is the most important aspect of management
If signs of anaphylaxis prescribe an Adrenaline Auto Injector and an Anti-Histamine. Guidance and doses can be found in the BNFc, Anaphylaxis Campaign and Resuscitation Council:
- https://bnfc.nice.org.uk/
- https://www.anaphylaxis.org.uk/hcp/what-is-anaphylaxis/medication/
- https://www.resus.org.uk/anaphylaxis/emergency-treatment-of-anaphylactic-reactions/
Referral information required
- Clear history of events and examination findings
- Drug implicated
- Strength/formulation/route
- Condition being treated
- Previous exposure history
- Time between administration of dose and onset of symptoms
- Number of doses before onset
NO testing is required prior to referral
Referrals should be directed to the paediatric allergy team at UHCW NHS Trust
Exclusion Criteria
The following groups of patients should be referred to General Paediatric clinics and NOT the allergy service:
- Infant feeding and possible Cow’s Milk Protein Intolerance (Very few children with reflux actually have an intolerance and true IgE mediated cow’s milk protein allergy is very rare – only 2.22% of children with a Cow’s milk intolerance have a true IgE mediated allergy )
- Urticaria with no identifiable allergen
Further information
Demand for allergy services nationwide is rising due to raised awareness of allergic conditions high profile cases in the media and an increase in the incidence of several types of food and airborne allergies.
Currently there is a 6 month waiting list for new patients
GP expediting of appointments is not possible except in children with true anaphylaxis (cardiovascular or respiratory compromise or altered conscious state as a result of exposure to an allergen).
Please bear this in mind when discussing appointments with patients.
Contacts
- Email: childrensallergy@uhcw.nhs.uk, we aim to respond within 1 week.
- Advice & Guidance: for clinical and referral advice
- Non-acute referrals: please send via E-Referral.
Useful websites:
The British Society for Allergy & Clinical Immunology (BSACI) www.bsaci.org
Anaphylaxis Campaign www.anaphylaxis.org.uk
www.bsaci.org
Itchy Sneezy Wheezy www.itchysneezywheezy.co.uk
www.eczemacareonline.org.uk
www.sparepensinschool.uk
Leave feedback
You must be logged in to post a comment.